Case Report: An elderly man with coronary artery disease and a pacemaker
A 72-year-old man with a history of hypertension, coronary artery disease, congestive heart failure, anxiety and a pacemaker presents to the emergency department for seven hours of non-radiating chest pain associated with dyspnea. He denies syncope, palpitations, fever, cough or other complaints. What's your diagnosis?


(©AfricaStudio,AdobeStock_140883501)



EKG


MI in the paced rhythm from "The Emergency Medicine 1-Minute Consult."
A 72-year-old man with a history of hypertension, coronary artery disease, congestive heart failure, anxiety and a pacemaker presents to the emergency department for seven hours of non-radiating chest pain associated with dyspnea. He denies syncope, palpitations, fever, cough or other complaints.
Exam: Vital signs are normal. Exam is normal. There is no jugular vein distention (JVD), abnormal heart sounds, pulmonary rales or peripheral edema.
Initial differential diagnosis:
- Anxiety
- Aortic dissection
- GERD
- Pulmonary Embolism
- Acute Coronary Syndrome
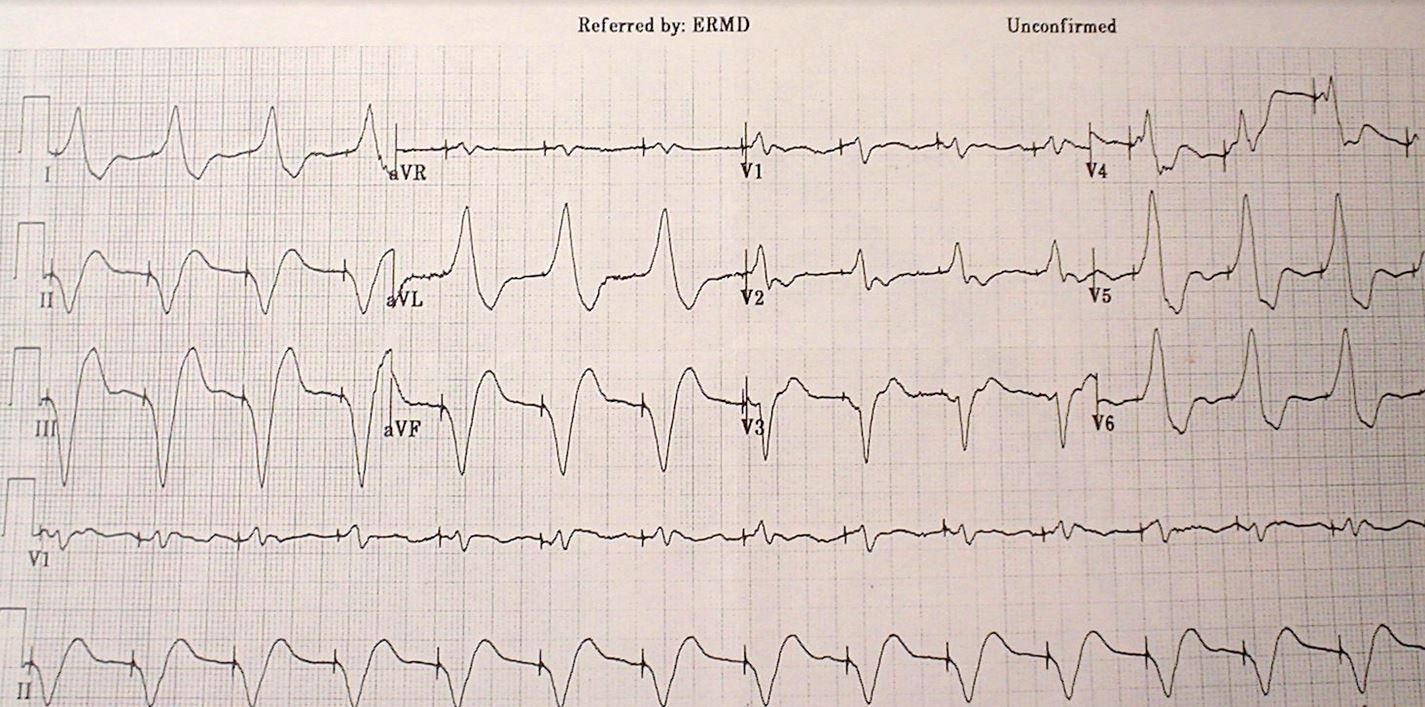
EKG read (see image on the right):
- Normal sinus rhythm
- Wolff-Parkinson-White
Do you agree with the read?
NEXT PAGE: Answer
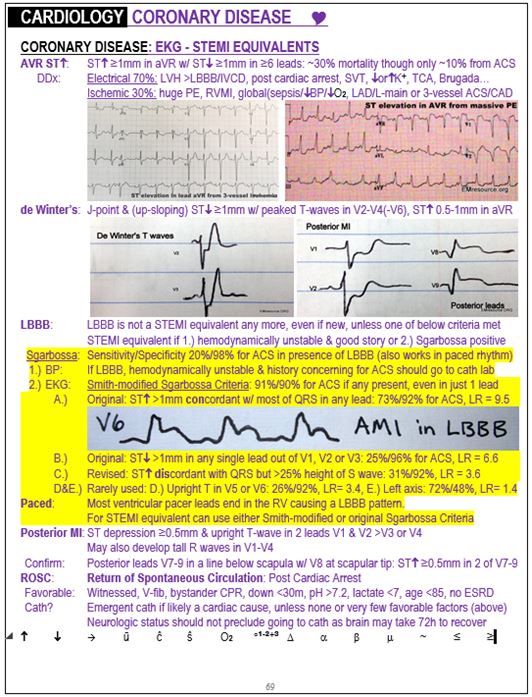
The computer read is incorrect as it is not picking up the pacer spikes properly. This occurs frequently. It is probably calling Wolff-Parkinson-White (WPW) syndrome because of the slow QRS upstroke which mimics a delta wave. What is more important is that this EKG is diagnostic of an inferior occlusion myocardial infarction (OMI) by the Smith-modified Sgarbossa criteria, which are explained in the sample page on the right. (Reviewed by Dr. Stephen W. Smith of Dr. Smith’s ECG Blog.)
DISCUSSION
It is more difficult for computers and health care providers to detect acute coronary syndrome in the presence of a bundle branch block or a paced rhythm. The Sgarbossa criteria were developed to help with this difficulty and the Smith-modified Sgarbossa criteria are an improvement over the original, with much better sensitivity (91% as opposed to 20%) with only a small loss of specificity (90% as opposed to 98%). See the highlighted area on the page to the right for more information. When two percentage numbers are listed, the first is sensitivity and the second is specificity.
CASE CONCLUSION
This patient went to the cath lab where the angiogram showed a 98% occlusion of the right coronary artery. Serial troponin-i’s resulted as follows: 4.9, 9.6, 4.2.
CASE LESSONS
- Use Sgarbossa or Smith-modified Sgarbossa criteria to diagnose STEMI in a paced rhythm.
- If you need more definitive EKG findings, consider using a magnet to temporarily disable the pacer and get an intrinsic rhythm EKG.
About the Author
Dr. Pregerson is chief editor of http://EMresource.org, an emergency medicine website that includes a free EM ultrasound library, EM cases of the month, EM pocket references and more.
Peer Review: Dr. Stephen W. Smith of Dr. Smith’s ECG Blog.















