The Quest for Ideal Kidney Function, with Kim Zuber, PA-C, and Jane Davis, DNP
Kim Zuber, PA-C, and Jane Davis, DNP, provide perspective on the new National Kidney Foundation and the American Society of Nephrology formula for calculating eGFR.
Loss of kidney function ranges from minimal impairment to kidney failure. Over time, scientists and medical researchers have proposed various formulas to enable providers to calculate function and direct medical treatment. Ideally, a measured glomerular filtration rate (mGFR) would provide this guidance.
However, this requires a continuous IV of a freely filtered substance secreted by the kidneys. The patient then collects a 24-hour urine and an accurate measurement of kidney function results. While accurate, this is expensive, time consuming, invasive and inconvenient for the patient and practitioner.
Substitute estimated measurements, or the estimated GFR (eGFR), were developed starting with the Cockrault-Gault (CG) in 1976.1 While CG was the standard for many years, it had drawbacks. The study cohort was made up of 249 hospitalized white males who were administered IV inulin (a freely filtered substance) with urine clearance monitored for 24 hours. Serum creatinine (SCr) is dependent on muscle mass and hospitalized patients are not representative of the general population. Furthermore, there were no women or patients of color and the number in the cohort was statistically insufficient.
Serendipitously, a study of dietary changes for the kidney patient ‘Modification of Diet in Renal Disease,’ published in 1999, used a different calculator that included both patients of color and females. This MDRD calculator had an African American (AA) adjustment based on the theory that AAs had more muscle mass than other groups.2 Initially the adjustment was 1.2; for example, a SCr of 1mg/dL in a white patient was equal to a SCr of 1.2mg/dL in the AA patient.3
In 2009, incorporating data from the African American Study of Kidney Disease (AASK) and the National Health and Nutrition Examination Survey (NHANES) trials, this racial adjustment was decreased to 1.16 in the CKD-EPI calculator.4 While it is widely known that SCr is dependent on muscle mass, less well known is the fact that these calculators did not control for musculature. Data collected in the 1970s may also be flawed due to the higher number of ‘blue-collar’ patients of color, the lack of amputees and/or athletes in the study cohort.
Although African Americans represent only 13% of the US population, they make up 35% of the patients with kidney failure. An AA person is four times more likely to develop kidney disease than a White person.5 In 2019, a group of medical students questioned why so many more Black patients developed ESKD.6 Is this a function of evaluation? Management? Genetics? Are we to blame? Or a combination of all the above? Students posed the question, “Why does the group of patients at highest risk have the highest eGFR? That simple question upended more than 50 years of evaluation and treatment of kidney disease.
In 2020, the National Kidney Foundation (NKF) and the American Society of Nephrology (ASN) convened a task force to investigate the removal of the race modifier in the eGFR calculator. They were tasked with deciding if race should be removed from the present calculator and if so, what new calculator could be applied across the board to patients with kidney disease.7
After a year of hearings, study, and input from stakeholders (labs, researchers, statisticians, practitioners, patients, government officials), the task force released the new eGFR calculator without the race modifier (CKD-EPI 2021).7 The new calculator increased the female, weight and height portion of the present calculator while removing race (Fig 1). While the new calculator was released in late 2021, implementation was to occur during 2022 with lab computer systems updated and a new billing code released.8
The Veteran’s Administration Hospitals moved to the new race neutral calculator in March 1, 2022. LabCorp® followed in May 2022, Quest® in June 2022 and major medical centers announced movement to the new calculator during summer 2022.9 In July 2022, the United Network of Organ Sharing (UNOS) stated that the eGFR without the race coefficient would be the standard used.10 Recently published studies have shown that the new race neutral calculator will shorten transplant wait times for patients of color by making them transplant eligible sooner.11
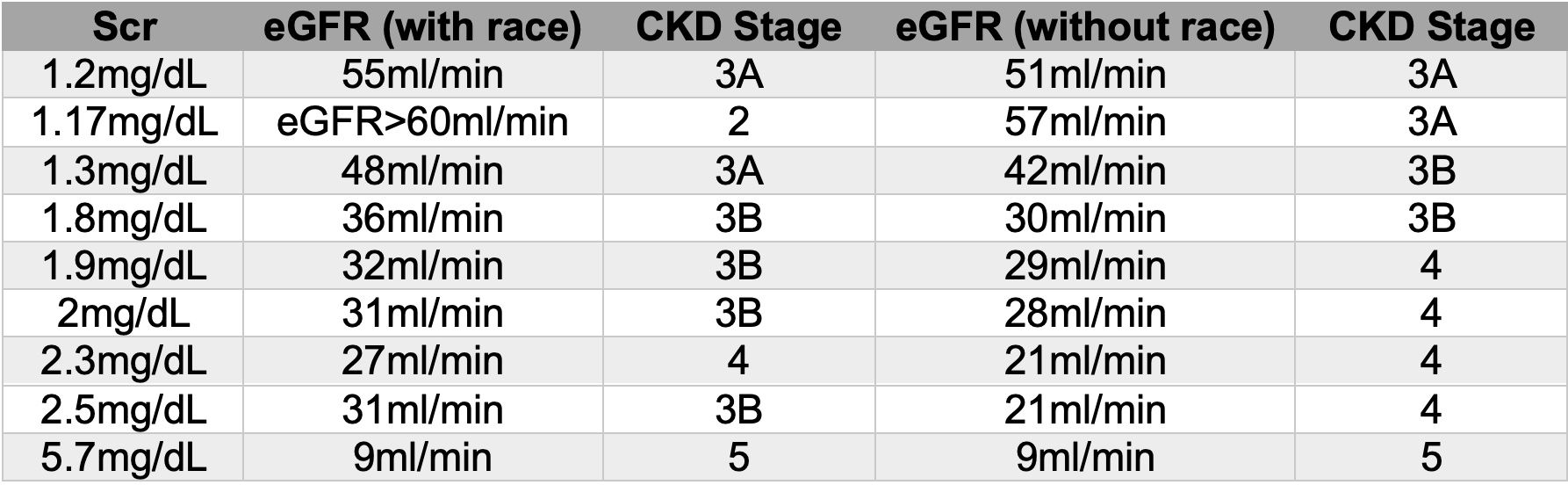
How has this change affected patients and practitioners? There are some unexpected results of the new equation. (Fig 2) Interpreting kidney function often involves studying trends. This may mean reviewing past creatinine values to determine how past eGFRs correlate with the new one. Many non-nephrology providers are unaware of the new calculator and become alarmed at the “decline” in kidney function. We have no way to compare the two eGFR calculations (old and new) and thus, we cannot direct our colleagues regarding trends except to state that the new calculator without the race adjustment is ‘more’ correct. It also reports values higher than 60ml/min as a specific number. This allows better quantification for the primary care provider who often treats the Stage 1-2 CKD patient.


Figure 2: Examples of patients using the old and new eGFR calculator
The easiest way to ascertain if your lab is using the new CKD-EPI 2021 calculator is to look at your recent eGFR reports or to call the lab manager. Some systems are using eGFRcr to differentiate the new calculator. Other systems are simply reporting just 1 result without the race modifier. The new formula can be accessed as a phone app via a free download at the app store or at: https://www.kidney.org/apps/professionals/egfr-calculator
Figure 1: Differences in eGFR calculators7
Old formula: CKD-EPI eGFRcr (CKD-EPI) (age, sex, race)
eGFR = 141 X min (Scr/κ, 1) α X max (Scr/κ, 1)- 1.209 X 0.993 Age X 1.018 [if female] X 1.159 [if black]
Where Scr is serum creatinine, κ is 0.7 for females and 0.9 for males, α is -0.329 for females and -0.411 for males, min indicates the minimum of Scr/ κ or 1, and max indicates the maximum of Scr/κ or 1.
______________________________
New formula: eGFRcr (CKD-EPI) refit without race variable
eGFR = 142 X min (Scr/k,1) α X max (Scr/k,1) - 1.200 0.9938 Age X 1.012 [if female]
where Scr is serum creatinine, k is 0.7 for females and 0.9 males, α is -0.241 for females and -0.302 for males, min indicates the minimum of Scr/k or 1, max indicates the maximum of Scr/k or 1.
References:
- Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31-41.
- Levey AS, Inker LA, Coresh J. GFR estimation: from physiology to public health. Am J Kidney Dis. 2014;63(5):820-834
- Levey AS, Bosch JP, Lewis JB, et al. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;130(6):461-470
- Levey AS, Stevens LA, Schmid CH, et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604-612.
- U.S. Renal Data System, USRDS 2016 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2016
- Eneanya ND, et al. Reconsidering the consequences of using race to estimate kidney function. JAMA 2019; 322:113–114
- Delgado C, Baweja M, Crews DC, et al. A Unifying Approach for GFR Estimation: Recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease. Am J Kidney Dis. 2022 Feb;79(2):268-288.e1
- Paul Palevsky, MD, NKF President, ASN special report, virtual ASN meeting, Nov 2021
- Paul Palevsky, MD, NKF President, oral update, NKF Spring Clinical Meetings, Boston April 2022
- United Network of Organ Sharing, implementation notice July 27, 2022, https://unos.org/news/implementation-notice-race-neutral-egfr-formulas/, Accessed 10Oct2022
- Ku E, Amaral S, McCulloch CE, Adey DB, et al. Comparison of 2021 CKD-EPI Equations for Estimating Racial Differences in Preemptive Waitlisting for Kidney Transplantation. Clin J Am Soc Nephrol. 2022 Sep 19:CJN.04850422









