Case Report: 52-year-old woman with MS and generalized weakness
A 52-year-old female with a history of multiple sclerosis presents to the emergency department for generalized weakness and trouble swallowing. Blood tests are ordered. Can you diagnose this patient?


(©Fizkes,AdobeStock_289879473), (©Logo3in1,AdobeStock_181735729)


Initial EKG read


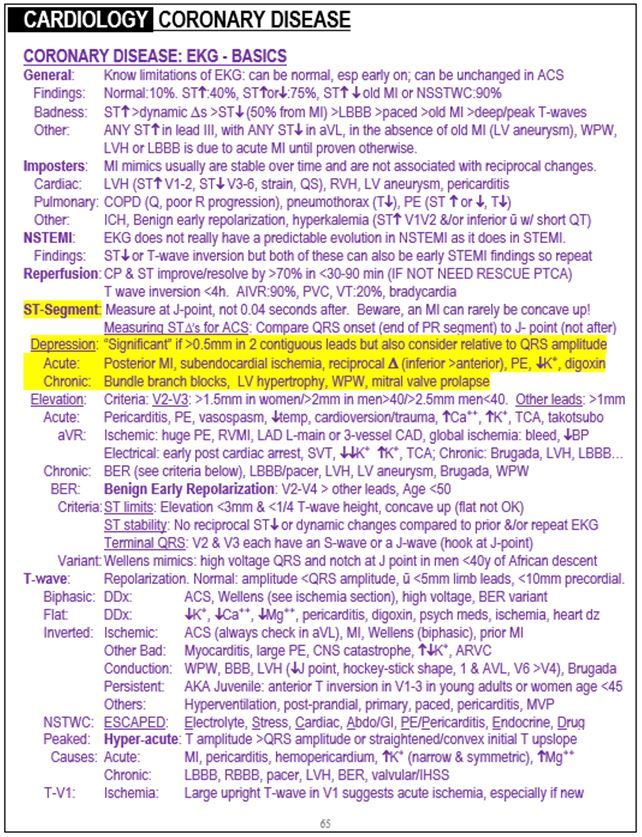
ST depression and hypokalemia excerpt from "The Emergency Medicine 1-Minute Consult "


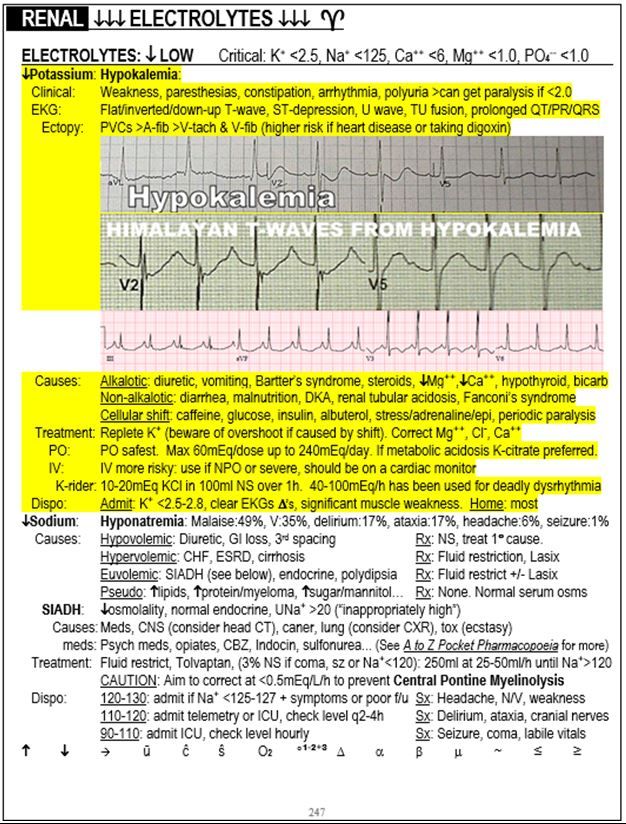
Electrolytes excerpt from "The Emergency Medicine 1-Minute Consult "
A 52-year-old female with a history of multiple sclerosis presents to the emergency department for generalized weakness and trouble swallowing that has gradually worsened over the past six days. She denies any syncope, palpitations, chest pain, dyspnea, fever, cough, sore throat or other complaints.
Exam: Vital signs are normal except for a pulse of 115 beats per minute. Blood pressure is 140/88. Ear nose and throat exam is unremarkable and she is handling secretions without difficulty. The rest of her physical exam is otherwise non focal.
Initial differential diagnosis: Tachydysrhythmia, electrolyte abnormality, pulmonary embolism, acute coronary syndrome.
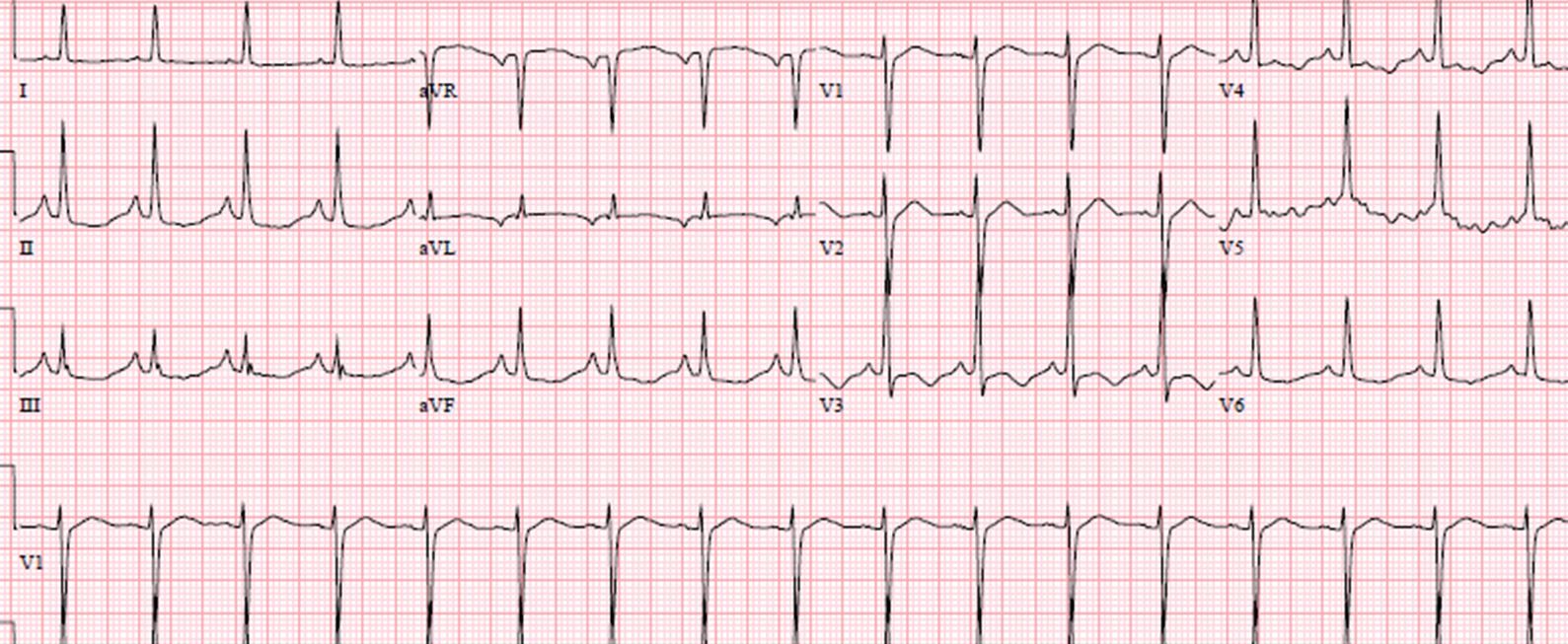
EKG read (see image on the right for initial EKG):
1. Sinus tachycardia
2. Right atrial enlargement
3. ST & T wave abnormality, consider inferior ischemia
4. ST & T wave abnormality, consider anterolateral ischemia
5. Abnormal ECG
Do you agree with the EKG read? What should you do next?
NEXT PAGE: Answer
EKG ANALYSIS
(Peer reviewed by Dr. Stephen W. Smith of Dr. Smith’s ECG Blog)
The computer read is correct. The ”right atrial enlargement” read is due to the large P-waves in leads II, III and aVF which is also known as P-pulmonale because it is usually due to chronic pulmonary disease, most commonly COPD. The “consider ischemia” read is due to slight ST depression and T-wave inversion in the anterio-lateral and inferior leads.
When the computer reads “consider ischemia,” it is important to always consider other conditions that cause ST depression and or T-wave inversion besides ACS: PE and hypokalemia are the main acute ones. Digoxin toxicity is another ones. LVH and bundle branch blocks are the main chronic ones, with WPW and MVP being less common causes. The computer printout will not put these in the differential diagnosis but you should.
This ECG is pathognomonic for hypokalemia. Only hypokalemia causes this sagging, scooped ST depression with a long QU-wave. Some call it a “wavy” pattern.
CASE CONCLUSION: Potassium level was 1.9 suggesting hypokalemia. The test was repeated to confirm the diagnosis. Magnesium level was normal.
The Emergency Medicine 1-Minute Consult: ST depression and hypokalemia (see second image on the right).
CASE LESSONS
Hypokalemia is the main cause of sagging, scooped out or wavy ST segment depression. There is often a U wave as well.
Here are links to two other interesting cases:
For any complaint, it is always wise to start with a broad differential diagnosis. Causes of painless acute generalized weakness and ischemic-looking EKG changes include more than just acute coronary syndrome. Consider the following:
- painless MI/ACS
- painless PE (about 20% of PE’s are painless, usually the larger ones)
- hypokalemia
- digoxin toxicity
About the Author
Dr. Pregerson is chief editor of http://EMresource.org, an emergency medicine website that includes a free EM ultrasound library, EM cases of the month, EM pocket references and more.
Peer Review: Dr. Stephen W. Smith of Dr. Smith’s ECG Blog.















